Nasotracheal intubation remains a valuable technique in anesthesia, oral and maxillofacial surgery, and critical care. While the overarching principles of nasal intubation are consistent across pediatric and adult applications, the procedure differs substantially between these populations due to different anatomical, physiological, and complication-related considerations. Literature comparing these groups underscores the importance of tailoring technique and decision-making to patient age.
The pediatric airway is uniquely challenging. Children have a proportionally larger tongue, a higher and more anterior larynx, and shorter tracheal length compared with adults. Narrow nasal passages increase the risk of trauma during tube passage, and even minimal misplacement can result in bronchial intubation or accidental extubation. Adults generally present with more predictable airway dimensions, and their wider nasal passages make passage technically easier, though trauma and sinus-related complications remain a concern.
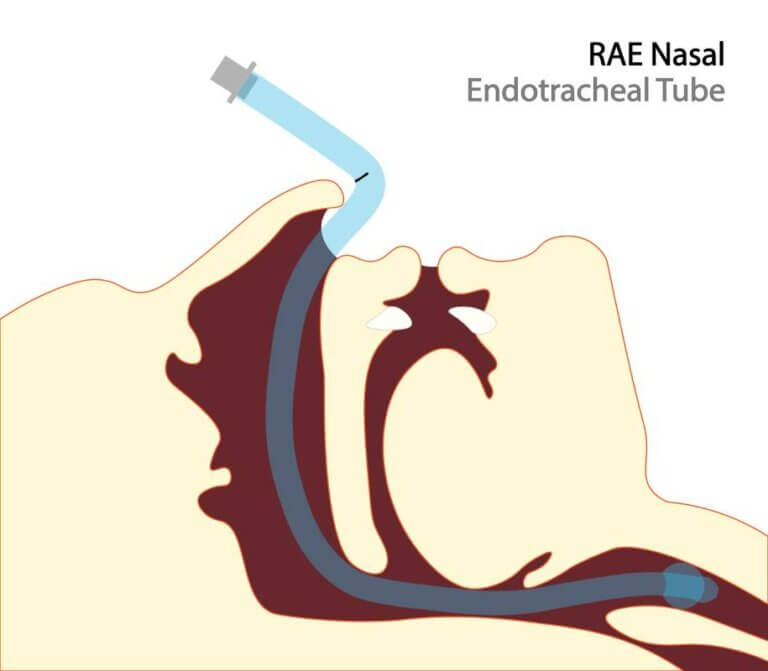
Tube selection and intubation strategy must reflect these anatomic differences in the nasal passageways between pediatric and adult patients. In pediatrics, strategies such as thermosoftened tubes, adequate lubrication, and the use of nasopharyngeal airways as guides help minimize mucosal injury. Fiberoptic bronchoscopy is often the preferred technique for infants and small children, particularly in difficult airway scenarios, but it requires availability of appropriately sized scopes and experienced operators. Adults more commonly benefit from video laryngoscopy-assisted or bougie-guided approaches, which have been shown to reduce trauma and increase first-pass success rates.
Epistaxis is the most frequent immediate complication across all age groups. Longer-term complications differ substantially. Adults are at higher risk of sinusitis, ventilator-associated pneumonia, and infectious sequelae during prolonged nasotracheal intubation. Pediatric studies suggest that neonates and infants may initially have lower rates of infectious complications compared with older children and adults, but the risk increases with longer intubation times.
Randomized controlled studies further define age-specific considerations. In critically ill children, there appears to be no significant difference in post-extubation airway obstruction between nasotracheal and orotracheal groups, though nasotracheal placement may provide superior tube security. In adults, bougie-assisted nasotracheal intubation under video laryngoscopy has been shown to significantly reduce both mucosal trauma and intubation time compared with unguided passage.
Operator experience plays an important role in outcomes. Comparisons of expert versus trainee performance in children under two years of age demonstrate that, with supervision, trainees can achieve success rates comparable to experts when using fiberoptic techniques. These findings reinforce the importance of structured training, particularly since pediatric nasal intubations are relatively infrequent in many institutions.
The choice of nasal versus oral intubation depends on surgical requirements, anticipated duration of ventilation, and patient-specific risk factors. Nasal intubation is often preferred when surgical access to the oral cavity is required or when tube stability is paramount. Contraindications include coagulopathy, basilar skull fractures, and unfavorable nasal anatomy. In pediatric patients, the narrow margin for error and higher risk of airway trauma necessitates meticulous technique and vigilant monitoring. In adults, the long-term infectious complications of nasal tubes are a central concern during prolonged ICU courses.
Nasotracheal intubation remains an essential airway tool, but its application differs significantly between pediatric and adult patients. Pediatric anatomy demands precise tube sizing and depth assessment, while adult patients face higher risks of infectious complications with prolonged use. Guided techniques, whether fiberoptic in children or bougie-assisted video laryngoscopy in adults, improve success rates and reduce trauma. Evidence also underscores the importance of training and supervision to ensure safe practice across age groups. Ongoing research is needed to establish standardized, evidence-based protocols that reflect the distinct risks and benefits in each population.
References
- Kim J, Jeon S. Nasotracheal intubation in pediatrics: a narrative review. J Dent Anesth Pain Med. 2024;24(2):81-90. doi: 10.17245/jdapm.2024.24.2.81
- Kumar V, Angurana SK, Baranwal AK, Nallasamy K. Nasotracheal vs. orotracheal intubation and post-extubation airway obstruction in critically ill children: an open-label randomized controlled trial. Front Pediatr. 2021;9:713516. doi: 10.3389/fped.2021.713516
- Greene NH, Jooste EH, Thibault DP, et al. A study of practice behavior for endotracheal intubation site for children with congenital heart disease undergoing surgery. Anesth Analg. 2019;129(4):1061-1068. doi: 10.1213/ANE.0000000000003594
- Jagannathan N, Sequera-Ramos L, Sohn L, et al. Randomized comparison of experts and trainees with nasal and oral fibreoptic intubation in children less than 2 yr of age. Br J Anaesth. 2015;114(2):290-296. doi: 10.1093/bja/aeu370
- Abrons RO, Zimmerman MB, El-Hattab YMS. Nasotracheal intubation over a bougie vs non-bougie intubation: a prospective randomized, controlled trial using videolaryngoscopy. Anaesthesia. 2017;72(12):1491-1500. doi: 10.1111/anae.14029